
Adductor strains are common complaints among professional and amateur athletes alike in soccer and can result in major time loss. Even though I treat and train a greater amount of soccer players compared to other sports, it is a common injury among ice hockey, running, football, lacrosse, etc and the mechanism is often the same.
The prevalence ranges between 2-3 in 10,000 in mens soccer in the NCAA and greater in men than women.¹ The most common mechanism is non-contact.¹ They can be complex problems with pain typically in the anterior-medial aspect of your thigh (front/inside) and referring down to the knee. Symptoms can be characterized as irritation, inflammation or tearing of muscle and/or tendon tissue. The most frequent mechanisms of injury are kicking (33%), change of direction (20%), stretch/reaching situations (17%), sprinting (15%), and jumping (7%). The primary reason these injuries occur is related to load tolerance and specificity of training relative to the demands of the sport. Load tolerance is effectively how much resistance, volume and stress tissue is trained to handle and manage. If a given movement or skill is above what the tissue was trained to handle, it fails and an injury occurs.
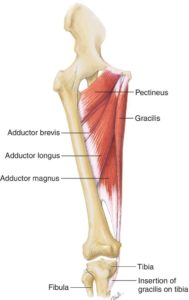
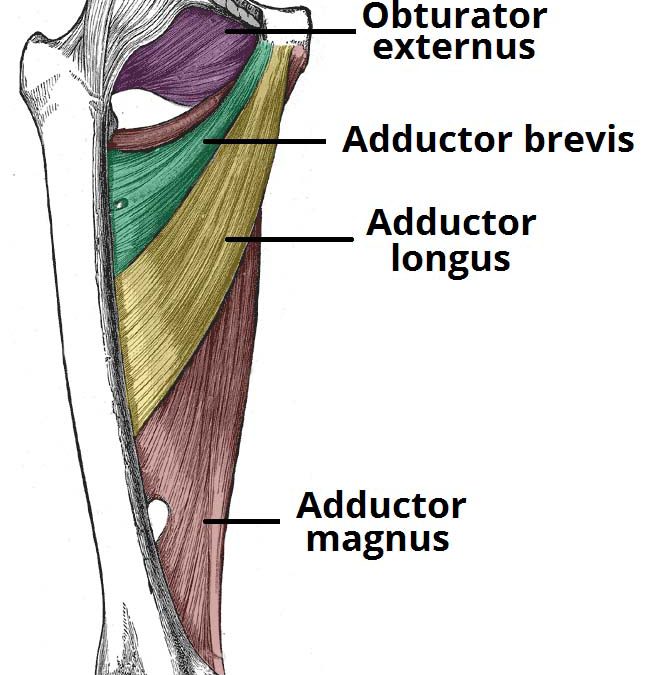
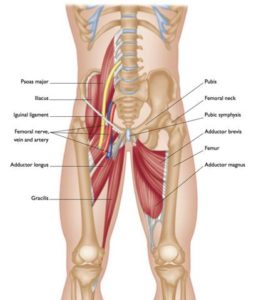
The adductor muscle group consist of the the muscles shown here on the left: pectineus, adductor brevis, adductor longus and adductor magnus and gracilis. These muscles run from the pubic bone and attach to various aspects along the femur, with the gracilis attaching on the tibia. Each of these muscles vary in function based on where they attach, however as a group their primary function is hip adduction (bringing the leg closer to the other leg). They also have a key role in changing direction as well as stabilizing the leg and pelvis in single leg positions (running, cutting and shooting). Furthermore, the pectineus and adductor brevis assist in hip flexion whereas the adductor magnus, longus and gracilis assist in hip extension.²
 Given flexion/extension are secondary actions, they not as strong compared to the primary movers in hip flexion/extension, injury can often times occur when performing the actions mentioned above.
Given flexion/extension are secondary actions, they not as strong compared to the primary movers in hip flexion/extension, injury can often times occur when performing the actions mentioned above.
Consider the job description of the adductor muscle group. They adduct the leg; they assist in stabilizing the pelvis; three help with extension of the hip; two help with flexion of the hip. There are a lot of jobs to coordinate, control and be trained.
Treatment and Training
If your goal is to play and improve your game, you aren’t all that valuable to your team while sitting on the sideline. What are you going to do about it?
Prior to starting any treatment or training, having a proper physical therapy and movement screen is a must. If you don’t know where to look and what to address, how could you possibly be successful? Rest alone is never the answer.
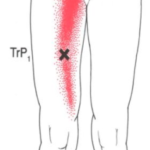
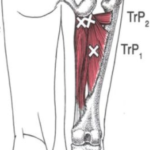
With adductor pain, the initial goal is controlling pain and removing it as quickly as possible. Pain will alter how you move, available range of motion, strength and motor control. With an adductor strain, we utilize strategies such as dry needling, soft tissue and instrument assisted soft tissue massage which can be very effective at removing pain and creating better tissue extensibility. Here are some referral patterns and trigger points of your adductor longus/brevis (left) and adductor magnus (right). The “x” is where common dysfunction is and red is where pain can refer to. As you can see here, pain oftentimes can refer to the knee/hip. This is why we do an in-depth screen to rule in/out what is going on.

As pain is being controlled, correcting movement dysfunction, motor control and building a structured strength and conditioning program is critical to return to play. Keep in mind that progress does not occur in isolation. Integrating range of motion, strength, agility, sprint training and nutrition all play important roles in the process.
There is no one size fits all training/rehab program for an injury which is why it is impossible to prescribe a training program in a post. That being said, there are specific qualities we look for when building out an individual athletes progress.
Considerations:
- Adductor and Abductor strength. There is strong evidence showing reduced adductor strength in those with pain compared to those without. Additionally, with weak glutes (abductors) you will have decreased strength and difficulty with pelvic control which will add additional stress/load upon your adductors (3,4). Here is a video of a great exercise for adductor strength that can be progressed from isometric (hold) to adding movement and control.
- Range of Motion (ROM). ROM and tissue extensibility are critical. With injury, we typically see restriction to movement as a protective mechanism. Adding additional motion through soft tissue work and end range movement will improve access and control to these limitations.
- Trunk stability. Reduced strength in the trunk and abdominal muscles can increase risk of injury here (3). If you cannot control your trunk/spine in relation to your pelvis and legs, it will set you up for more than just an adductor injury. Being able to control your trunk is a critical aspect of sport and performance leading to progress in injury prevention, better movement mechanics and increased speed!
- Multi-Planar Movement. There must be integration of multi-planar movement in all 3 planes: sagittal (front/back), frontal (side-to-side) and transverse (rotational). Incorporating combined movement into programing is key. Since we now know some of the adductors assist in flexion and extension at the hip, building in movements that encourage this is a must. It also adds foundations of change of direction work required for soccer. Doing so through lunge variations and med ball work are just two of many ways to do so.
- Strength. Do you remember we discussed one of the reasons for injury is the amount of load your body can manage? Improving overall strength through lower, trunk and upper body will improve muscle strength and control as well as improve tolerance to the stress and load put on your body. Customizing this based off of assessment, role on the soccer field and injury background are just a few ways we prioritize and program.
- Specificity. Once you have laid the foundation, you need to put all the pieces together. Adding field based rehab, agility, strength and conditioning is essential to progression into game play. Reintroducing sport specific load to the previously injured tissue continues to prepare your body to tolerate the demands of full practice and game situations.
Take Home
As you can see, rehab and training after an injury is not general and should be comprehensive. If you have had or are currently managing an adductor strain, get assessed, learn your strengths and your limitations and start addressing it. We look for key qualities in movement to reduce risk of injury, improve movement, strength and performance to build better athletes. Keep in mind the structure of your rehab/training, and the timing for when and why to include certain aspects of rehab/training.
Sign up for our FREE Newsletter
Recieve performance physical thearpy, nutrition and training tips!
You have Successfully Subscribed!
References
- Eckard, T. G., Padua, D. A., Dompier, T. P., Dalton, S. L., Thorborg, K., & Kerr, Z. Y. (2017). Epidemiology of Hip Flexor and Hip Adductor Strains in National Collegiate Athletic Association Athletes, 2009/2010-2014/2015. The American Journal of Sports Medicine,036354651771617. doi:10.1177/0363546517716179
- Branci, S., Thorborg, K., Nielsen, M. B., & Hölmich, P. (2013). Radiological findings in symphyseal and adductor-related groin pain in athletes: a critical review of the literature. British Journal of Sports Medicine, 47(10), 611-619. doi:10.1136/bjsports-2012-091905
- Kloskowska, P., Morrissey, D., Small, C., Malliaras, P., & Barton, C. (2016). Movement Patterns and Muscular Function Before and After Onset of Sports-Related Groin Pain: A Systematic Review with Meta-analysis. Sports Medicine, 46(12), 1847-1867. doi:10.1007/s40279-016-0523-z
- Ishøi, L., Sørensen, C. N., Kaae, N. M., Jørgensen, L. B., Hölmich, P., & Serner, A. (2015). Large eccentric strength increase using the Copenhagen Adduction exercise in football: A randomized controlled trial. Scandinavian Journal of Medicine & Science in Sports, 26(11), 1334-1342. doi:10.1111/sms.12585